
Bone marrow oedema
Pathology
Bone marrow edema (BME) is typically identified via MRI or ultrasound when a patient has another condition or pain in or around the bone. Most frequently, they occur in the hip, knee, ankle, or foot but can occur in all bones.
It`s a relatively frequent disease, although its prevalence has yet to be examined further. In a recent study of patients with foot and/or ankle pain the prevalence of bone edema in MRI was 23%. There, the average patient was male, aged approximately 50, with traumatic or degenerative origin talus bone edema.1
In many cases, the liquid inside the bone will go away with time, therapy, and pain medication, such as nonsteroidal anti-inflammatory drugs (NSAIDs). However, waiting for the edema to go away by itself can take a long time, which is especially concerning for professional athletes, but also frustrating for regular patients. From practical cases, we know that exclusively focusing on avoiding load and exercises, unfortunately only brings limited success. Therefore, a better approach is needed and has been investigated in recent research groups.
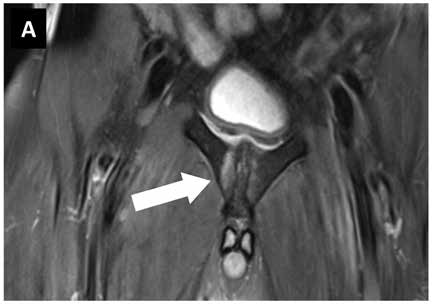
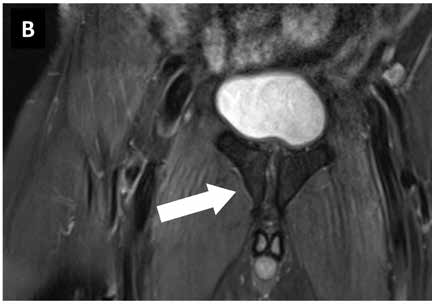
Images: MRI pubic bone branch football player 1st German Bundesliga. (A) Findings before start of therapy with focused ESWT, (B) findings 6 weeks later with no pain under stress.
Images courtesy of sportärztezeitung.
Causes:
Painful bone marrow edema can occur spontaneously or secondary to various, underlying diseases. Therefore, the detection of edema in the bone marrow is important in managing symptoms of arthritis, stress fracture, cancer, or infection. It can indicate where the pain started and how strong the bones are, which in turn will affect the treatment choice. Common causes of bone marrow edema include:
- Injuries: such as plantar fasciitis or tendinitis
- Stress fractures: Stress fractures occur with repetitive stress on the bones. This can occur due to physical activity such as running, competitive dancing, or weightlifting. The fractures are characterized by bone edema and fracture lines.
- Arthritis: Bone edemas are relatively common in those who have both inflammatory and noninflammatory arthritis. It’s usually due to a cellular infiltrate within the bone which compromises bone cell function and appears as the disease gets worse together with loss of cartilage
- Cancer: Metastatic tumors can produce a higher water production in bone. This edema will appear in ultrasound or MRI. Radiation treatment can also cause edemas to occur.
- Infection: Swollen tissues can cause increased water in the bone. The edema will typically go away after the infection is treated.
Treatment
The most important therapeutic measure is the research into the cause of the bone marrow edema or the stress reaction/ stress fracture of the bone. Thus, triggering events, unaccustomed stress or incorrect stress should be investigated.
Initial treatment is symptomatic with restricted weight bearing, analgesics, and physiotherapy. In addition, corticosteroids, bisphosphonates, and prostaglandin inhibitors are used. Although BME is usually self-limiting, previous conservative therapy has not been successful in shortening the course of the disease. To research more effective approaches, recent publications have highlighted more holistic approaches. For example, an interdisciplinary task force was set up within our large osteology center at the Ludwig Maximilian University in Munich, Germany, consisting of specialists from internal medicine, endocrinology/diabetology, hematology/oncology, orthopedics, pediatrics, physical medicine, radiology, rheumatology, and trauma surgery to develop a consensus paper. You can read more on their findings under this link.

Extracorporeal shock wave therapy (ESWT) has also shown to be a promising addition for a conservative treatment approach. Practical evidence shows its effectiveness in various orthopaedic diseases (Kienböck's disease, plantar fasciitis, osteitis pubis, osteonecrosis of the femoral head). In general, shock wave therapy promotes the self-healing powers of the tissue and can therefore be a useful tool in managing underlying diseases or other, relevant symptoms.
Specifically, in bone tissue, this means the stimulation of osteoblasts and periosteum cells and the differentiation of stem cells. It is assumed that there is an increased secretion of nitric oxide synthase and vascular endothelial growth factor, which could lead to increased angiogenesis. In addition, the periosteum is stimulated and the activity of osteoclasts is reduced. To summarize, shock wave therapy promotes the treatment of the underlying causes around the pathology of bone marrow edema, to activate the bone structure to heal itself.
Evidence
The first evidence that ESWT can support the treatment of a bone marrow edema was established in a study by Steinborn et. al. in 2000: Extracorporeal shock wave application for chronic plantar fasciitis associated with heel spurs: prediction of outcome by magnetic resonance imaging. There, in a group of patients with chronic plantar fasciitis who also had a confirmed calcaneal bone marrow edema on pretherapeutic MRI, ESWT delivered positive, satisfactory clinical outcomes.2
In addition, a systematic review by Häußer et al. provided a summary of the history of the treatment of osteonecrosis of the femoral head, showing bone bruises, with focused shock wave therapy.3 Further information on this study can be found via our partner Sportärztezeitung.
Further relevant studies demonstrate that the Swiss DolorClast® is useful in a treatment protocol for bone bruise was published by Duan et. al. from Chongqing, China. 4,5
References:
1) González-Martín D, Herrera-Pérez M, Martín-Vélez P, Rendón-Díaz D. Prevalence of bone marrow edema in a study population with foot and/or ankle pain. Foot (Edinb). 2019 Sep;40:76-80. doi: 10.1016/j.foot.2019.04.004. Epub 2019 Apr 17. PMID: 31136917.
2) Extracorporeal shock wave application for chronic plantar fasciitis associated with heel spurs: prediction of outcome by magnetic resonance imaging.
Maier M, Steinborn M, Schmitz C, Stäbler A, Köhler S, Pfahler M, Dürr HR, Refior HJ.
J Rheumatol. 2000 Oct;27(10):2455-62. PMID: 11036844.
3) Häußer, J., Wieber, J. & Catalá-Lehnen, P. The use of extracorporeal shock wave therapy for the treatment of bone marrow oedema — a systematic review and meta-analysis. J Orthop Surg Res 16, 369 (2021). https://doi.org/10.1186/s13018-021-02484-5
4) Cao J, Zhang C, Huang H, Yang L, Duan X. Bone Marrow Edema Syndrome of the Foot Treated with Extracorporeal Shock Wave Therapy: A Retrospective Case Series. J Foot Ankle Surg. 2021 May-Jun;60(3):523-528. doi: 10.1053/j.jfas.2020.10.007. Epub 2020 Oct 7. PMID: 33573900.
5) Zhang C, Huang H, Yang L, Duan X. Extracorporeal Shock Wave Therapy for Pain Relief After Arthroscopic Treatment of Osteochondral Lesions of Talus. J Foot Ankle Surg. 2020 Jan-Feb;59(1):190-194. doi: 10.1053/j.jfas.2019.07.015. PMID: 31882139.
Treatment Procedure - example of Osgood Schlatter disease
Locate the area of pain through palpation and biofeedback.
Mark the area of pain.
Apply coupling gel to transmit shock waves to the tissue.
Deliver Radial or Focused Shock Waves to the area of pain while keeping the applicator firmly in place on the skin.
Clinical proof
Practitioner?
Get information on the diagnosis, the functioning of shock wave therapy, clinical proof, contraindications, etc.
Recommended settings
Discover our products
