
Subacromial Pain Syndrome
Pathology
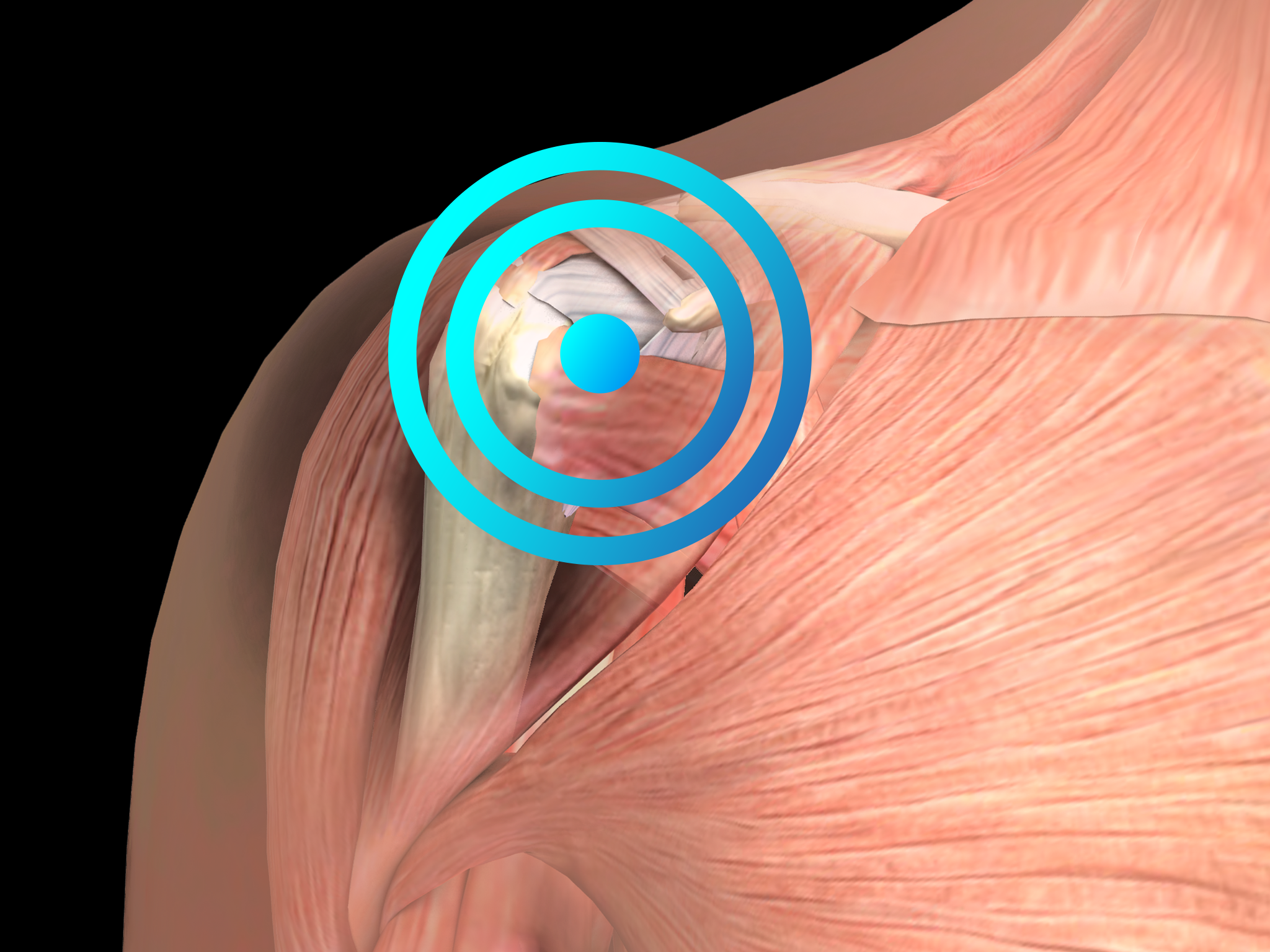
As calcifying tendinitis of the shoulder (details are provided in the corresponding Section) can also present with shoulder pain, the subacromial pain syndrome can also comprise calcifying tendinitis of the shoulder. Sometimes the term rotator cuff tendonitis is confused with the term shoulder bursitis, but both terms refer to an inflammation of a particular area within the shoulder joint (i.e., the subacromial space) that is causing a common set of symptoms and is named shoulder impingement syndrome (SIS). The term SIS is descriptive and refers to pinching of the tendons and bursa of the rotator cuff between bones (i.e., in the subacromial space). In most acute cases SIS is a combination of inflammation of the rotator cuff tendons (tendonitis) and inflammation of the bursa that surrounds these tendons (bursitis). In many cases of SIS the subacromial space is reduced because of the different shape of the bones compared to healthy control people.
The condition is often caused by an initial injury, starting the inflammatory process. This may cause thickening of the tendons or bursa, taking up more space and pinching these structures even more, resulting in more inflammation.
Accordingly, the problem can be self-exacerbating, resulting in a vicious circle of inflammation, thickening of the tendons and bursa, pinching of these structures, more inflammation, and so on.
Diagnosis is based on the clinical features of the disease. Diagnostic imaging should be considered to rule out other causes of shoulder pain (including calcifying tendinitis of the shoulder) or to establish the diagnosis of SIS when in doubt.
Shoulder impingement syndrome (SIS) is the most common form of shoulder pain, and repetitive activity at or above the shoulder during work or sports (including swimming, throwing, tennis, weightlifting, golf, volleyball, and gymnastics) represents the main risk factor for SIS. Increasing age predisposes to SIS.
With respect to therapy, three different stages of SIS are distinguished:
- Stage 1 (acute inflammation, edema, and hemorrhage in the rotator cuff): conservative treatment including rest, icing, physiotherapy, and nonsteroidal anti-inflammatory drugs.
- Stage 2 (continuum of Stage 1, with the rotator cuff tendon progressing to fibrosis and tendonitis): conservative treatment, radial shock wave therapy (RSWT), or surgery when conservative treatment and RSWT fail.
- Stage 3 (mechanical disruption of the rotator cuff tendon and/or changes in the coracoacromial arch with osteophytosis along the anterior acromion): surgery.
Radial shock wave therapy can be a very effective element of shoulder impingement syndrome treatment.
Side effects of Radial Shock Wave Therapy (RSWT®) using the Swiss DolorClast®
When performed properly, RSWT® with the Swiss DolorClast® has only minimal risks. Typical device-related non-serious adverse events are:
- Pain and discomfort during and after treatment (anesthesia is not necessary)
- Reddening of the skin
- Petechia
- Swelling and numbness of the skin over the treatment area
These device-related non-serious adverse events usually disappear within 36h after the treatment.
Treatment Procedure
Locate the area of pain through palpation and biofeedback.
Mark the area of pain.
Apply coupling gel to transmit shock waves to the tissue.
Deliver Radial or Focused Shock Waves to the area of pain while keeping the applicator firmly in place on the skin.
Clinical proof
Recommended settings
Discover our products
