
Greater trochanteric pain syndrome
Pathology
The main clinical symptoms are pain and reproducible tenderness in the region of the greater trochanter and/or the buttock or lateral thigh. The diagnosis is based on the clinical features of the disease. Diagnostic imaging should be considered to rule out other causes of hip pain or to establish the diagnosis of Greater trochanteric pain syndrome when in doubt.
The greater trochanter is the site of attachment for the tendons of five muscles: the gluteus medius and gluteus minimus laterally, and the piriformis, obturator externus and obturator internus medially. As in the shoulder, injury and subsequent degeneration may occur in the components of the rotator cuff of the hip, starting with tendonitis, tendinosis, and eventual tear. This process occurs more commonly in the gluteus medius than the gluteus minimus.
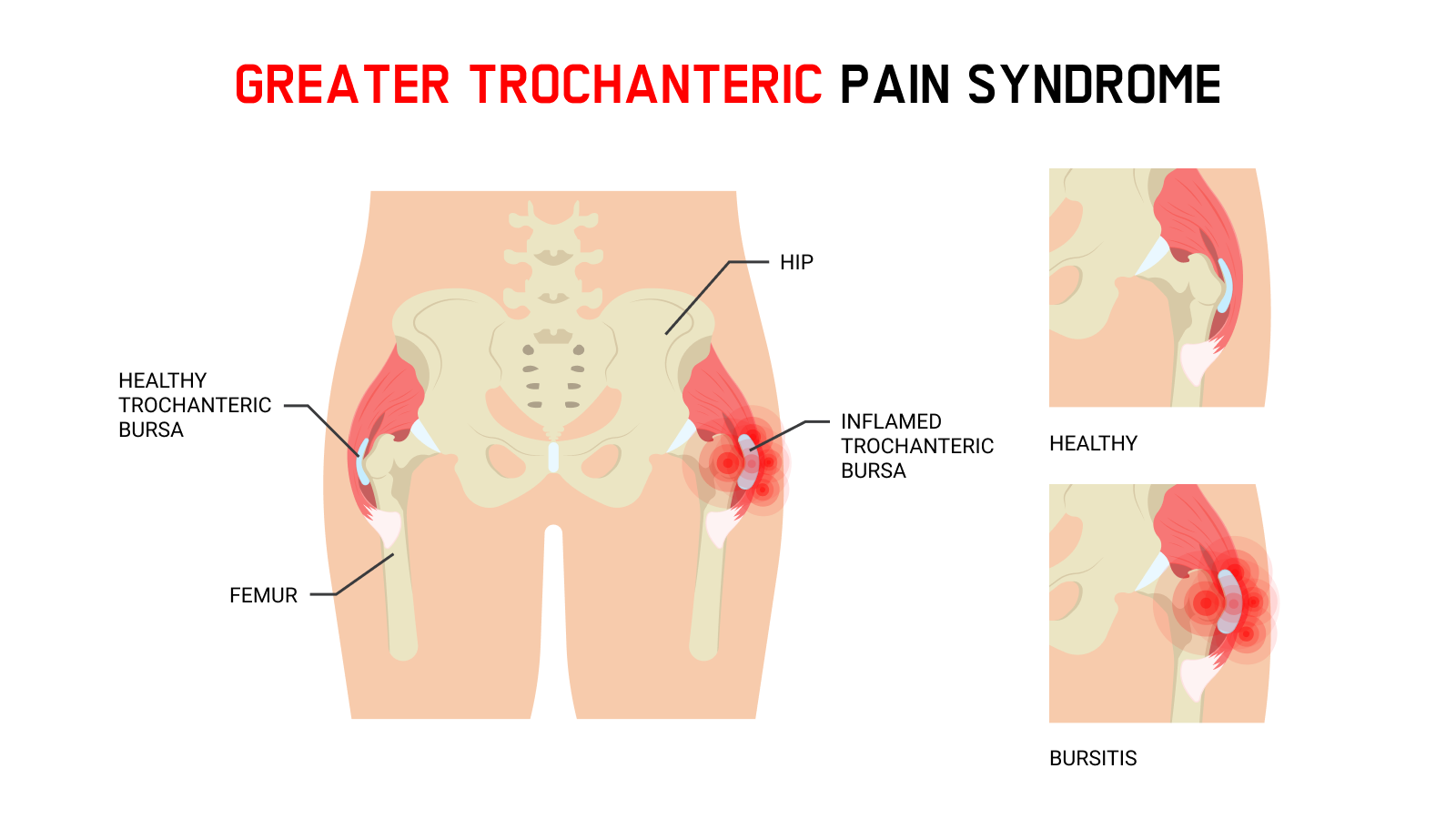
Furthermore, there are three bursas present around the lateral aspect of the greater trochanter, i.e., the subgluteus maximus bursa, the subgluteus medius bursa and the gluteus minimus bursa. These bursas are believed to serve as cushioning for the gluteus tendons, the iliotibial band, and the tensor fascia latae. Trochanteric bursitis mostly occurs secondary to repetitive friction between the greater trochanter and the iliotibial band with hip flexion and extension. Trochanteric bursitis is also often associated with overuse, trauma, or other conditions that may alter normal gait patterns.
Greater trochanteric pain syndrome has been reported to affect between 10% and 25% of the general population, with an increased prevalence in women compared to men.
Therapy of symptomatic tendon tears comprises rest, anti-inflammatory medications and physiotherapy focusing on a range of motion and strengthening exercises. Trochanteric bursitis is usually self-limiting and responds to rest, ice, anti-inflammatory medications and physiotherapy focusing on stretching, flexibility, strengthening and gait mechanics. When symptoms persist despite these interventions, bursal injections of local anaesthetics and corticosteroids can provide effective pain relief.
Radial shock wave therapy has been demonstrated to be efficient for recalcitrant greater trochanteric pain syndrome.
In the case of the inefficacy of RSWT, surgical intervention may be considered in cases in which other potential sources of the patient’s symptoms have been ruled out.
Side effects of Radial Shock Wave Therapy (RSWT) using the Swiss DolorClast®.
When performed properly, RSWT with the Swiss DolorClast® has only minimal risks. Typical device-related non-serious adverse events are:
- Pain and discomfort during and after treatment (anaesthesia is not necessary)
- Reddening of the skin
- Petechia
- Swelling and numbness of the skin over the treatment area
These device-related non-serious adverse events usually disappear within 36h after the treatment.
Treatment Procedure
Locate the area of pain through palpation and biofeedback.
Mark the area of pain.
Apply coupling gel to transmit shock waves to the tissue.
Deliver Radial or Focused Shock Waves to the area of pain while keeping the applicator firmly in place on the skin.
Clinical proof
Practitioner?
Get information on the diagnosis, the functioning of shock wave therapy, clinical proof, contraindications, etc.
Recommended settings
Discover our products
